
UK pandemic modelling, an update

In an earlier post, I outlined the model that I had built to try to understand how the pandemic in the UK might develop over the course of 2021, given assumptions about lockdown restrictions and the rollout of vaccines. I said in the post that I would try to keep the assumptions up to date as events unfold, and also asked for feedback on the model and the assumptions. Thank you to all those who gave me feedback, which was very helpful. In this post I will outline what has been built into the new, improved, “version 2”.
But first, let’s take a quick look at how the predictions from version 1 stacked up against the data that has been published over the last nine days.
How did I do?
The first key prediction was around the speed of vaccination rollout. I was sceptical of how well the government would do here and so assumed a starting rate of 0.5 million vaccinations a week, ramping up to 2 million over the following 30 days. The good news is that they have done much better. The initial rate was 1 million per week and that increased up to about 2.2 million per week within four days. By 17th January, a total of 4.3 million doses had been delivered, compared to the 2.5 million in my model by that date. I am very happy that my assumptions were too conservative here.
On deaths, I had predicted 85,312 by 17th January and the actual figure is 89,261. When it comes to the number of people in hospital, the latest data from the government is from the 14th January and shows 37,475 whereas my model predicted 32,091. So in both cases, things have been a little worse. I did say in my previous article that the lags in the system are probably bigger than accounted for in my model and I think that is what is driving the difference. Given that the daily case numbers have been rather more steady recently, I think that will be less of an issue going forward.
When it comes to case numbers, I predicted newly reported cases a day starting off at 56,000 and declining gradually to around 52,000 by now. I am pleased to say that the average over that period has been a little lower at 49,000/day and with a clear downward trend. So it looks like the lockdown measures are being slightly more effective than I had assumed, which is good news.
Enhancements to the model
The first area where I felt the model needed improvement was what level of immunity to assume for people who had recovered from COVID. I assumed full immunity but in the last few days a paper has been published which looked at this issue based on healthcare workers in the UK and and concluded that prior infection was estimated to provide an 83% protection against becoming reinfected. So I have now built this assumption into the model.
The second area where I have made changes is in properly modelling the two dose vaccination regime. Previously I had only tracked first doses and assumed a 70% effectiveness. I am now modelling both doses. As before, 70% effectiveness is assumed after the first dose but this is increased to 83% (same level as natural immunity) after the second dose. I have set the maximum gap between first and second doses at 12 weeks, so from around the middle of April the number of first doses drops significantly as constrained supplies of vaccine start having to be used to deliver second doses.
Another refinement to the vaccination assumptions is to reflect the fact that not everyone will be eligible for the vaccine (children 12 years old or younger) and some will be unwilling to get vaccinated. The proportion who will refuse to get vaccinated is obviously a key assumption which I will come back to later in this article.
The final set of model enhancements relate to the suppression policy. In version 1, I applied a fixed suppression rate throughout the forecast period, with 70% as the base assumption and I also looked at 65%. In reality, we know that the government will start to relax restrictions once the case rate drops, so I can now adjust suppression factors during the forecast period. In the scenarios I am sharing here, those adjustments take place on fixed calendar dates.
Other assumption changes
I have obviously refreshed the starting values for deaths and case numbers. One of the key assumptions is what proportion of the population is infectious at the start of the simulation. Previously, I used a figure of 2% of the population (1 in 50), based on the ONS prevalence survey. An updated estimate should have been provided by now - it is usually updated weekly but the release scheduled for the 15th January has been delayed due to delays in laboratory tests. A cynic might suspect that it contains good news about falling infection rates and the government wants to maintain maximum pressure to comply with the restrictions.
In any case, I’ve decided to switch to an alternative source for estimated prevalence, the COVID Symptom Study. This is kept constantly updated and seems very reliable to me. So I have used their figure of 726,341 symptomatic cases and grossed it up to allow for an estimated third of cases being asymptomatic, giving me an estimate of 1.1 million current cases in the UK.
The other thing that has moved on is vaccinations. There are two key assumptions, the take-up rate and the delivery rate.
Vaccination take-up
Based on recent survey evidence, the UK is likely to have one of the highest take-up rates in the world, as this chart from YouGov shows.

I’ve assumed that 15% of the population refuse to be vaccinated, the 11% “no’s” and just less than 50% of the “don’t knows”. In the model, I’ve assumed these people are all in the lower risk category.
Vaccination delivery rate
In public, the government is talking about every adult in the UK getting at least a first dose of the vaccination “by September”. Based on my calculations, they should hit that milestone by the start of September, even if the vaccination rate stays where it is at 2.2m/week, allowing for the 15% refusers. It would take them to the end of September if all adults got vaccinated, so maybe that is why they are being a little vague.
The chart below shows what happens if they run at a fixed rate of 2.2m/week and stick to a maximum 12 week gap between the doses. The vaccination programme will have to shift to doing only second doses during mid April to the end of June. It will only be from the start of July that they can resume giving first doses.

Of course, the government is working to increase the vaccination rate from the current levels. Media reports say that privately the government believes it can be delivering 4 to 5 million doses a week “within months”. I’ve assumed that they do succeed in doing that and the rate increases smoothly up to 4m/week over 90 days.
In that scenario, shown in the next chart, it is still a bit “start stop”, but generally with a higher rate of vaccination, it is possible to continue the momentum of first doses whilst also doing second doses on time. Crucially, the programme also arrives at the finishing line sooner. The whole (willing) adult population will have got at least their first shot by mid June and both doses a month later.

Suppression policies
The next topic is what approach the government will take to relaxing the lockdown.
Like before, I have assumed that the lockdown is delivering a 70% suppression of R at the moment. Together with my other assumptions, that gives me an effective R at the start of the simulation of 0.9.
The government has made it clear that they will prioritise reopening of schools. Based on estimates of the impact of schools being open on transmission levels, I think reducing the suppression factor to about 60% should be consistent with reopening schools. I’ve assumed that happens after half term, i.e. around the 22nd February.
I’ve then assumed a further big drop in suppression to 40% in mid April (“after Easter”) and then another drop to 20% in mid July, reflecting some minor ongoing restrictions and behavioural changes such as mask wearing on public transport.
Results
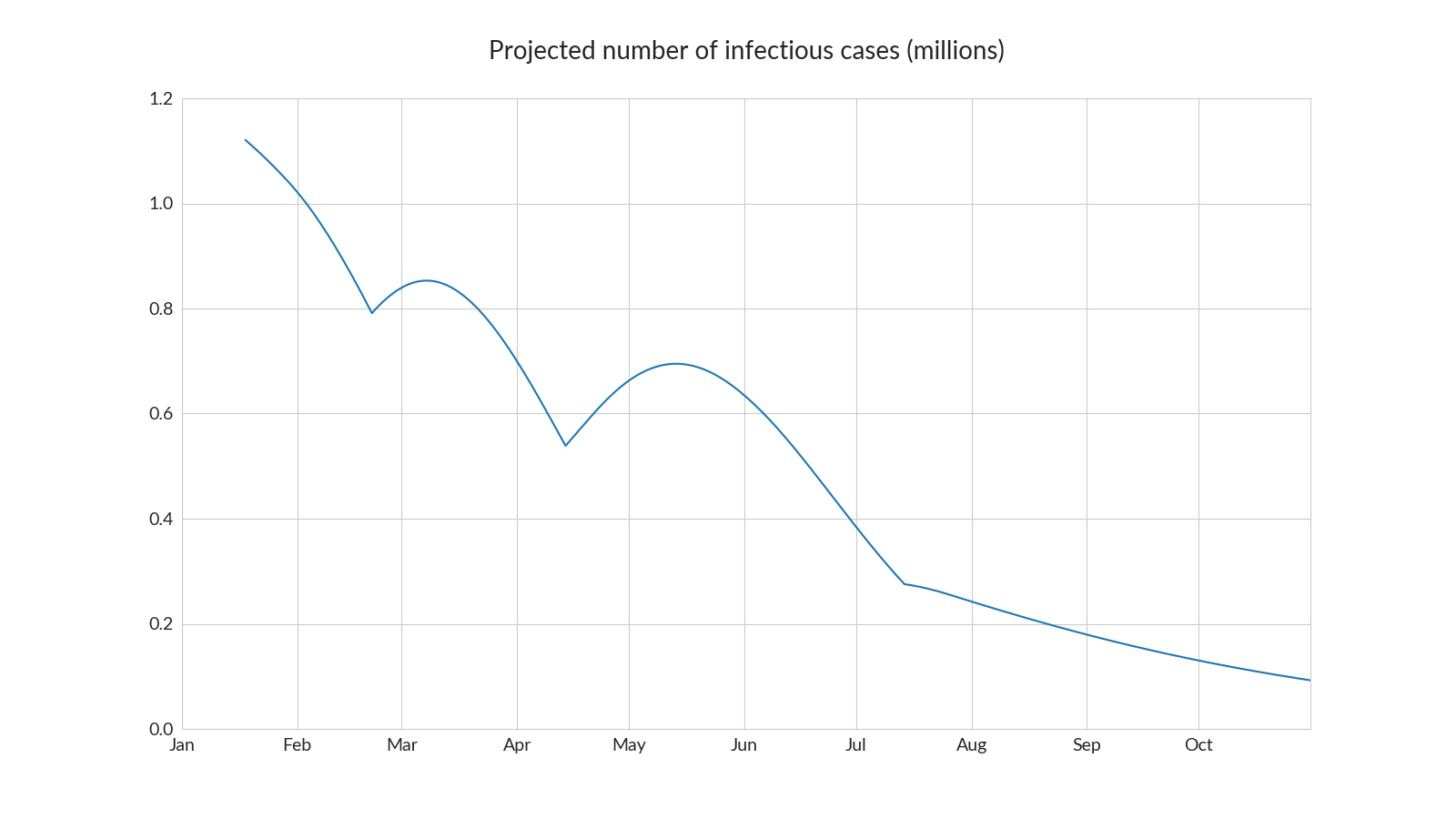
The projected number of infectious cases with all these assumption changes is shown on the following chart.
You can see that the sudden relaxations of restrictions that I have modelled cause something of a bumpy ride for case numbers, suggesting that this schedule of relaxation is a little too fast, with a series of “mini waves” ensuing after every relaxation. However, infections do start to come down again naturally within a few weeks as the vaccination programme continues to roll out. Of course in reality the relaxation will be done in a more gradual, phased way, but I do think this simulation shows that a relaxation schedule a bit like this may be feasible, especially if phased in regionally based on case levels.
What if we stay in lockdown longer? I’ve also modelled a policy which delays reopening schools until the start of April and pushes the next relaxation back six weeks to the start of June (next chart). That gives a much smoother and sustained reduction in cases. There are 7 million fewer cases in this scenario, with 16,500 fewer deaths. Interestingly, the smaller number of cases means that natural immunity is lower at the end, so R is actually slightly above one at the end of the simulation - i.e. we don’t quite achieve herd immunity.
By the standards of the figures we’ve become used to seeing every day, 16,500 deaths that may not sound like a lot. Many would argue that restricting people’s freedoms, hurting our children's education and killing the economy for an extra six weeks isn’t the right trade-off. But with high risk people vaccinated early on, many of those deaths will be less skewed towards the very old, and it is still more than five 9/11s after all.

What does this mean for aviation?
If my assumptions are correct about the vaccination efficacy, take-up, levels of immunity conferred by catching COVID and the rate at which the vaccination programme can be rolled out, then we do just reach herd immunity right at the end of programme, i.e. by September. So as long as new variants don’t come along to spoil the party, whatever policy path we take over the next few months, we should be out of the pandemic by then in the UK. Case numbers should be much lower by the summer too and, combined with seasonal effects that I haven’t really allowed for, perhaps things will feel much more “back to normal” by then.
But with the higher levels of transmission of the new variant, it is quite a close run thing to get to herd immunity. If more than 15% of adults refuse the vaccination, it may be impossible to reach it (except by a lot more people getting the disease of course). Vaccinating children would help, especially during periods when schools are open. At the moment, the UK is ahead of most other countries in the speed of its vaccination programme and the population seems one of the least “vaccine sceptical”. On the other hand the prevalence of the new variant works against bringing case numbers down. If the variant hasn’t already spread across the world, the rest of the world may keep the UK isolated for quite some time.
I think that will mean that travel restrictions and mandatory testing of some sort are likely to be in place for much of this year. Certainly the next few months are going to be grim. Personally, I would expect that we will see a recovery in travel after Easter which will build over the course of the year. I do believe there is a lot of pent up demand and once people are vaccinated, the fear factor will be much diminished. Of course, they do need to be allowed to travel, which depends on decisions from politicians all across the world.
The first half of 2021 looks like it is going to be a bumpy ride. I’m still hopeful that the second half will be very different, but given how rapidly things are changing, maybe that is too early to call.